 Skip to content
Skip to content 
Fatty liver in women is increasingly common, including in those who do not drink alcohol and those who are not overweight. Many women discover fatty liver incidentally during routine ultrasound scans despite normal liver enzymes. This article explores the hormonal and metabolic drivers behind fatty liver disease in women, why standard blood tests may miss early liver fat accumulation, why some women do not respond to generic lifestyle advice, and what evidence-based strategies support true fatty liver reversal.
Fatty liver in women is not simply a liver disorder.
It is a metabolic signal of underlying insulin resistance and metabolic dysfunction.
Quick Summary
- Fatty liver can develop even with normal weight and zero alcohol intake.
- Insulin resistance is the primary driver.
- Estrogen shifts significantly influence liver fat accumulation.
- Normal ALT and AST do not exclude fatty liver.
- PCOS, hypothyroidism, perimenopause, and chronic stress increase risk.
- Early stages are often silent and reversible.
- Metabolic repair works better than aggressive restriction.
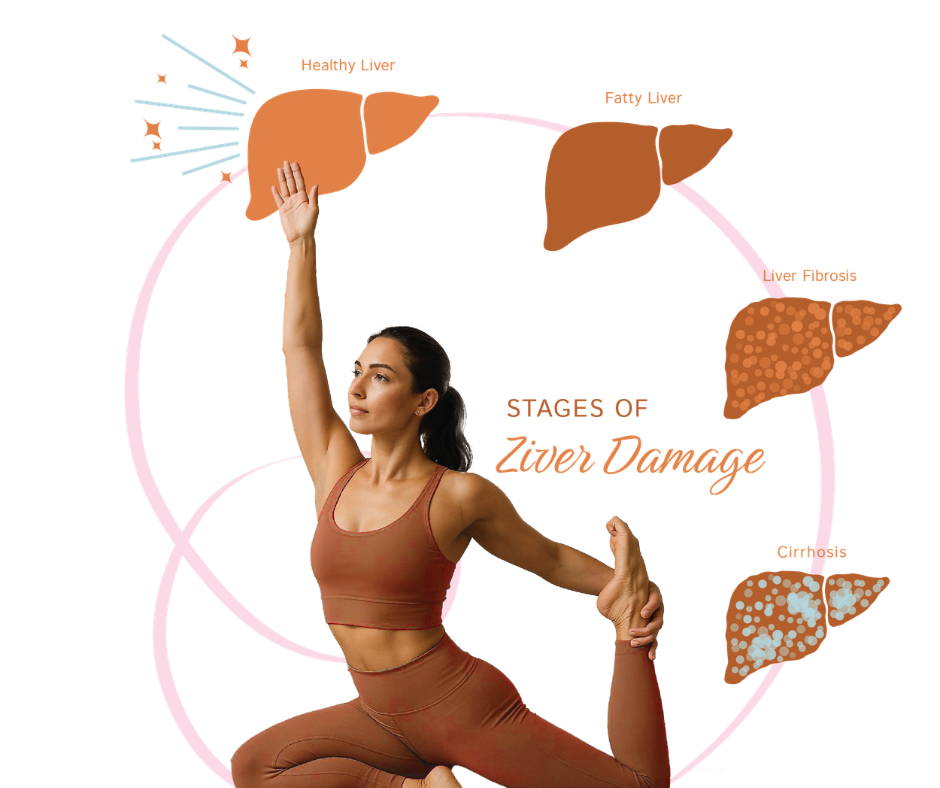
What Is Fatty Liver?
Fatty liver, now termed Metabolic Associated Fatty Liver Disease (MAFLD), refers to excess fat accumulation in liver cells in the presence of metabolic dysfunction and insulin resistance.
It is not primarily an alcohol condition in most women.
It is a reflection of insulin resistance, hormonal shifts, metabolic overload, and impaired liver fat metabolism.
Progression is not inevitable.
Early stages of fatty liver are highly reversible when the underlying metabolic drivers are addressed.
Why Fatty Liver Is Rising in Women
Historically associated with alcohol use in men, fatty liver disease is now strongly linked to metabolic dysfunction, insulin resistance, and hormonal imbalance.
Women are particularly vulnerable during:
- Perimenopause and menopause due to declining estrogen
- Polycystic ovary syndrome (PCOS)
- Thyroid dysfunction and hypothyroidism
- Post pregnancy insulin resistance
- Chronic stress and sleep deprivation
Estrogen enhances insulin sensitivity, supports mitochondrial fat oxidation, and limits hepatic lipogenesis. Its decline removes important metabolic protection against fatty liver development.
Women with Polycystic Ovary Syndrome (PCOS) have significantly higher prevalence of fatty liver, independent of BMI. Insulin resistance and hyperandrogenism contribute to hepatic fat accumulation.
Elevated fasting insulin and HOMA-IR (Homeostatic Model Assessment of Insulin Resistance) are strong predictors of fatty liver and metabolic liver dysfunction.
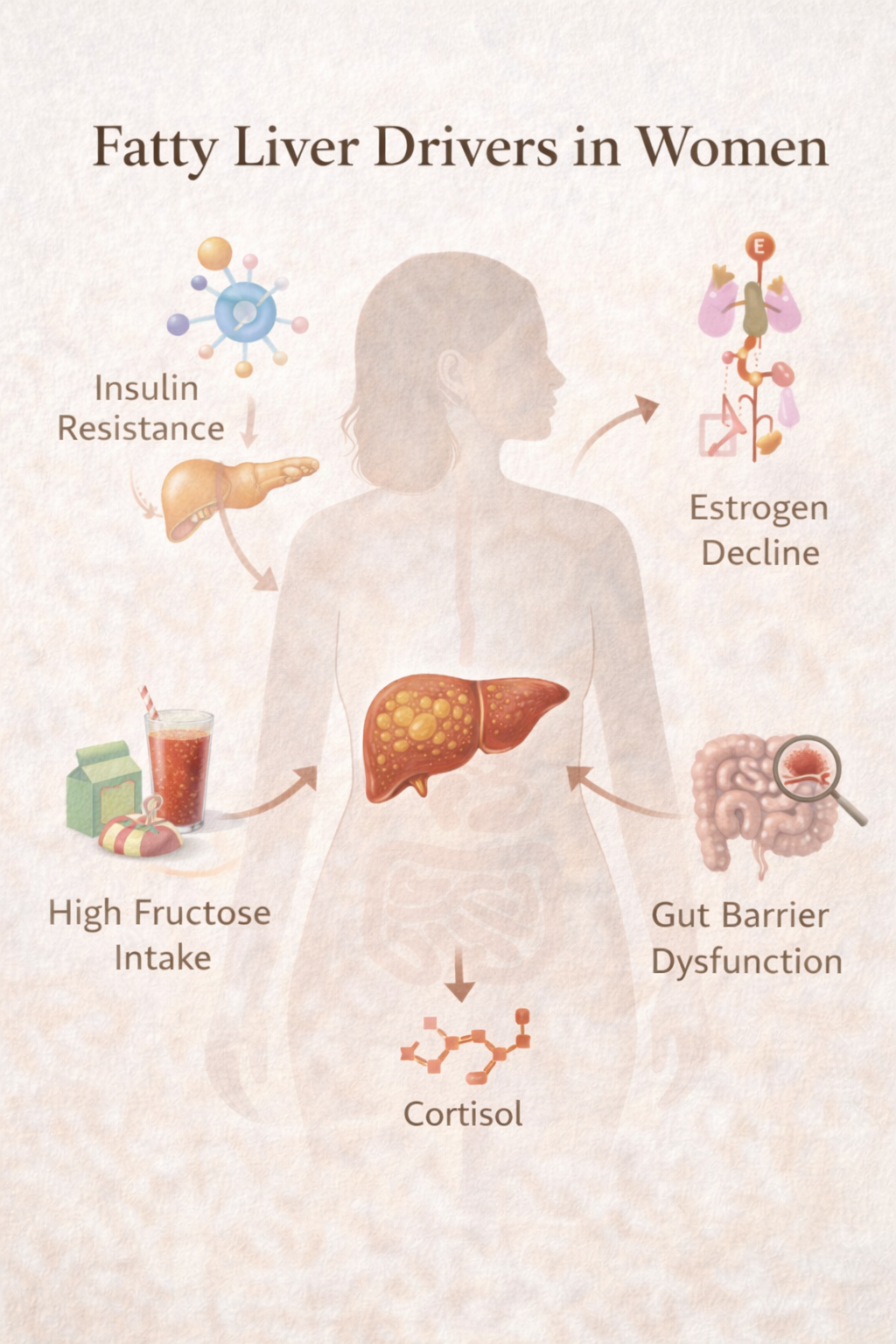
The Core Drivers in Women
Insulin Resistance
Excess glucose is converted into fat within the liver through de novo lipogenesis, increasing intrahepatic fat accumulation.
This process often precedes abnormal fasting glucose and HbA1c.
Elevated fasting insulin and HOMA-IR (Homeostatic Model Assessment of Insulin Resistance) are strong predictors of fatty liver and metabolic liver dysfunction.
Estrogen Decline or Imbalance
Estrogen regulates lipid metabolism and mitochondrial function.
Lower estrogen states increase visceral fat accumulation and hepatic fat storage, raising the risk of fatty liver in women during perimenopause and menopause.
High Fructose Intake
Fructose is metabolized primarily in the liver.
Excess intake from fruit juices, sweetened beverages, and ultra-processed foods increases hepatic triglyceride synthesis and liver fat accumulation, independent of total calorie intake.
Gut Barrier Dysfunction
Increased intestinal permeability allows endotoxins such as lipopolysaccharide (LPS) to reach the liver via portal circulation.
This activates inflammatory pathways and accelerates progression from simple steatosis to metabolic steatohepatitis.
Chronic Stress and Cortisol
Cortisol increases hepatic gluconeogenesis and promotes visceral fat accumulation.
Sleep deprivation further worsens insulin resistance, inflammation, and metabolic liver stress.
Why Normal Blood Tests Can Miss It
ALT and AST may remain within laboratory reference ranges in early fatty liver.
Important markers include:
- ALT elevation even within high-normal ranges
- AST to ALT ratio trends
- Gamma-glutamyl transferase (GGT) as an oxidative stress marker
- Triglycerides
- Fasting insulin
- HOMA-IR
Imaging tests such as ultrasound or FibroScan often detect fatty liver before liver enzymes rise.
Normal liver enzymes do not rule out early metabolic dysfunction or fatty liver.
How Fatty Liver Progresses and How Care Changes
Fatty liver exists along a continuum.
Metabolic dysfunction often begins before liver fat becomes visible on imaging.
As disease progresses, inflammation and fibrosis may develop.
Care is required at every stage. The difference lies in intensity and supervision.
Stage | What Is Happening | Primary Goal | Nutrition Foundation | Supplement Support | Supervision |
Metabolic Risk Phase (Pre-Steatosis, not an official stage) | Hyperinsulinemia and increased hepatic de novo lipogenesis begin before visible fat accumulation | Prevent hepatic fat deposition | Adequate protein, resistance training, carbohydrate pairing, reduce ultra processed foods, sleep correction | Magnesium if insulin resistant, ensure dietary choline, correct vitamin D deficiency | Monitor metabolic markers |
Stage 1 – Steatosis | Steatosis with low grade inflammation | Reduce liver fat and improve insulin sensitivity | Structured protein intake, fructose reduction, whole foods, high fibre, omega 3 rich foods | Omega 3 1 to 2 g EPA DHA, choline 250 to 500 mg if low intake, magnesium 200 to 400 mg | Periodic imaging and labs |
Stage 2 – Steatohepatitis (MASH/NASH) | Fat with active inflammation and oxidative stress | Lower oxidative stress and protect hepatocytes | Continue Stage 1 fully, strict glucose stability, no alcohol | NAC 600 to 1200 mg, milk thistle 140 to 300 mg silymarin, omega 3 therapeutic dose, vitamin D optimisation | Closer monitoring of enzymes and FibroScan |
Stage 3 – Fibrosis | Scar tissue formation from chronic inflammation | Prevent progression and support remodeling | Maintain metabolic correction, preserve muscle mass, avoid restrictive dieting | Structured antioxidant and anti inflammatory protocol under medical supervision | Regular hepatology follow up |
Stage 4 – Cirrhosis | Advanced structural distortion and functional compromise | Prevent decompensation and muscle loss | Adequate protein to prevent sarcopenia, balanced meals, avoid severe restriction, sodium moderation if indicated | Only under specialist care | Active specialist management |
Why Two Women Show Different Severity
Similar weight and lifestyle do not guarantee similar liver outcomes.
Differences are influenced by:
- Genetic variants such as PNPLA3 polymorphisms
- Muscle mass and metabolic rate
- Gut microbiome diversity
- Thyroid function
- Sex hormone balance
- Micronutrient status, especially choline, magnesium, and B vitamins
Choline is particularly critical for hepatic fat export via very-low-density lipoprotein (VLDL) synthesis. Inadequate intake increases fatty liver risk, especially in women with certain genetic variants.
Why Generic Advice Often Fails
Weight loss alone does not correct metabolic signaling or insulin resistance.
Severe calorie restriction may worsen metabolic stress in women with:
- Hypothyroidism
- Chronic stress
- Low muscle mass
- History of restrictive dieting
Muscle is a primary glucose disposal site. Loss of muscle mass reduces insulin sensitivity and worsens hepatic fat accumulation.
Metabolic restoration requires:
- Adequate protein intake
- Resistance training
- Sleep regulation
- Stress reduction
- Stable blood glucose patterns
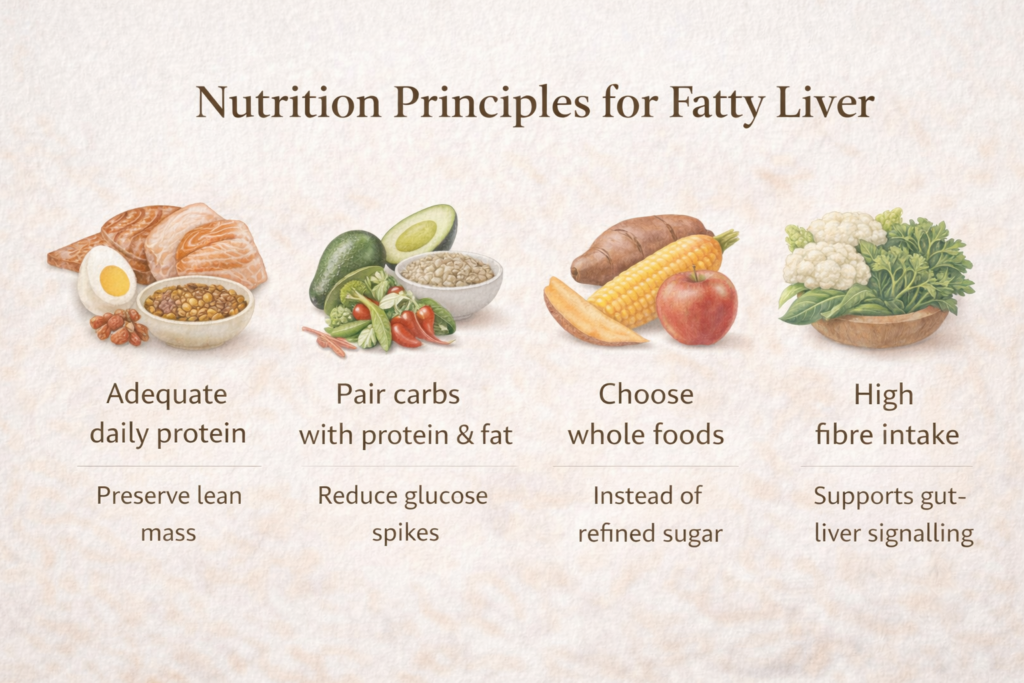
Nutrition Principles
Across stages of fatty liver disease, foundational strategies include:
- Adequate daily protein to preserve lean mass
- Pairing carbohydrates with protein and fat to reduce glucose spikes
- Choosing whole food carbohydrates rather than refined sugars
- Moderate use of healthy fats
- High fibre intake to support gut-liver signaling
- Regular resistance training
Include bitter and cruciferous vegetables such as radish, arugula, methi leaves, broccoli, cabbage, and cauliflower. Sulfur-rich vegetables support bile flow, estrogen metabolism, and hepatic detox pathways.
Clinical trials show that meaningful liver fat reduction can occur within 8–12 weeks with structured dietary and exercise interventions in early fatty liver.
Targeted Supplement Support (Inflammatory Stage)
Used when inflammation or oxidative stress is present. Not a replacement for diet.
- NAC (600–1200 mg): Supports glutathione production and reduces oxidative stress
- Omega-3 (1–2 g EPA + DHA): Reduces hepatic triglyceride synthesis
- Choline (250–500 mg if intake low): Supports liver fat export
- Magnesium (200–400 mg): Improves insulin sensitivity
- Silymarin (140–300 mg): Hepatoprotective support
Supplements support biology.
Nutrition, metabolic repair, and muscle preservation drive fatty liver reversal.
When to Seek Medical Evaluation
Most early fatty liver cases can be managed with structured metabolic care. Medical evaluation is important if you notice:
- FibroScan values persistently above 8 kPa
- Liver enzymes that remain elevated over time
- Type 2 diabetes with fatty liver
- Worsening metabolic markers despite lifestyle correction
- Strong family history of advanced liver disease
Urgent care is required if you develop yellowing of eyes, persistent abdominal swelling, unusual bruising, or confusion.
Stage 3 and Stage 4 fatty liver require coordinated medical supervision alongside nutrition and metabolic support.

The Key Takeaway
Fatty liver in women is rarely about alcohol.
It is a reflection of insulin resistance, hormonal shifts, chronic stress, metabolic overload, and impaired metabolic health.
Early stages are common and reversible.
Progress is reflected in improved insulin markers, reduced central fat, better energy, and hormonal stability.
The liver has remarkable regenerative capacity when metabolic biology is respected.
FAQ
Can you have fatty liver with normal weight?
Yes. Lean individuals with insulin resistance or PCOS can develop fatty liver, often called lean fatty liver disease.
Are normal liver enzymes reassuring?
Not completely. Early fatty liver frequently presents with normal ALT and AST.
Does fatty liver worsen hormonal imbalance?
Yes. The liver metabolizes estrogen and thyroid hormones. Liver dysfunction can amplify hormonal irregularities.
Is fatty liver reversible?
Stage 1 and early Stage 2 fatty liver are often reversible with targeted metabolic correction.
Does stress contribute?
Chronic cortisol elevation increases hepatic fat storage and insulin resistance.
Disclaimer: This article is for educational purposes only and is not a substitute for personalized medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before starting any supplement or therapy.


